Mental health clinics wait on Congress
If federal lawmakers don’t renew a promising program before the end of June, it will be up to the states to find the money

The promise of higher federal Medicaid payments is giving eight states the chance to show that one-stop mental health clinics with 24-hour crisis care could offer patients a better option than the de facto safety net of police departments and emergency rooms.
But the two-year experiment is drawing to a close now, leaving the program with an uncertain future if Congress doesn’t extend it.
In Missouri, clinics receiving the enhanced rates substantially boosted their staffing levels. The number of counselors and social workers at these clinics increased by around one-third, and the number of child psychiatrists rose by more than two-thirds. With more staff, the clinics saw a 20 percent increase in the number of people served each month, a 30 percent increase in total appointments and a 25 percent decrease in waiting times.
Debra Walker, director of public and legislative affairs at the Missouri Department of Mental Health, said the results mean more people receive same-day or next-day care when they need it.
“This enhanced access to care is expected to both improve consumer outcomes and to reduce costs in other parts of the health care, social services, law enforcement and judicial systems,” she said.
If Congress doesn’t renew the expiring program before the end of June, it will be up to the states to find the money to keep the enhanced payments flowing. Since states face tighter budget restrictions than the federal government, that could mean scaling back some services.
“If we’re unable to find a solution, we absolutely will have to decrease access to care,” said Laura Heebner, the executive vice president of Missouri’s Compass Health Network, one of the providers receiving the enhanced funding. “And that’s been the story of our lives.”
Also watch: What if we switch to a single-payer health care system?
[jwp-video n=”1″]
In recent years, around one-third of adults with serious mental illness and half of all adults and teens with any mental illness did not receive any kind of treatment, according to the Substance Abuse and Mental Health Services Administration, part of the U.S. Department of Health and Human Services.
The most common reason, cited by around a quarter of adults who didn’t get treated, was not knowing where to go for services. Privacy and perception concerns are also common.
So in 2014, Congress created a pilot program for one-stop mental health service centers that could meet a variety of needs and provide treatment. They’re modeled in part on federally qualified health centers, which similarly provide preventive and treatment services for physical conditions regardless of a patient’s ability to pay.
In addition to the 24-hour access, the behavioral health centers must meet other standards to qualify for the enhanced Medicaid payments. The staff must have not only diverse disciplinary backgrounds, but cultural and linguistic backgrounds that would meet the community’s needs. They must have relationships with other kinds of health clinics and psychiatric facilities to ensure seamless transitions across a range of health services.
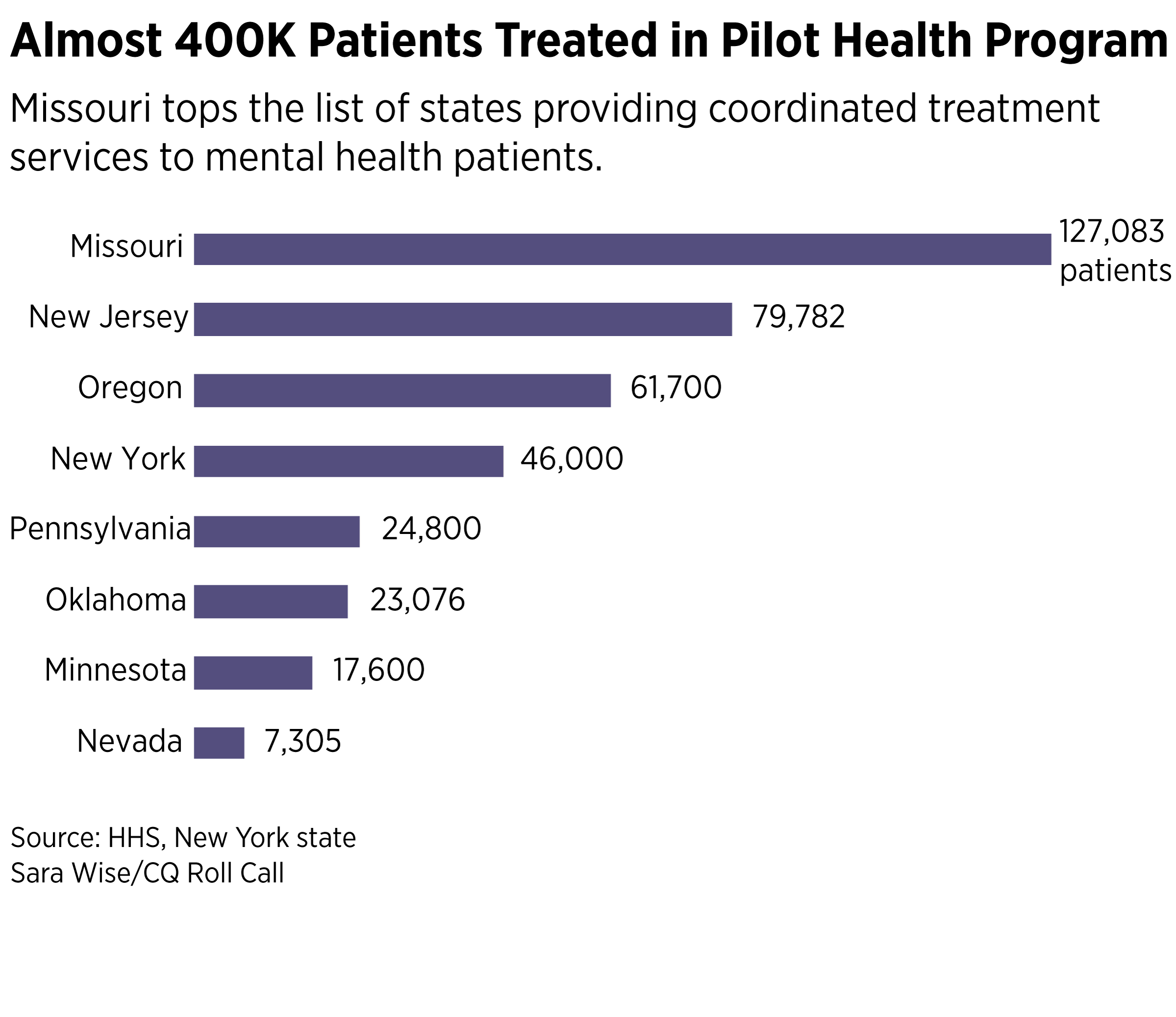
Across the eight selected states, HHS estimates that 372 locations will serve a total of around 381,000 individuals, including about 270,000 Medicaid recipients.
The issue has lawmakers’ attention. In two states that started the program earlier — Oklahoma and Oregon — the expiration date was supposed to be at the end of March. A bill signed into law on April 18 bought the programs three more months in those states.
Still, all eight states now face a deadline just a few months before the federal government’s enhanced funding for the clinics ends. Bills in Congress would extend the program — known as Certified Community Behavioral Health Clinics, or CCBHCs — for another two years and expand it to additional states. But as the hundreds of thousands of extra people that would be served would put the bill’s price tag above $1 billion, it would probably have to be included in a broader package where it could be balanced out by other cost-saving measures.
The bill’s supporters, representing a wide variety of states and political views, are optimistic.
“It’s an important part of the health care delivery system in the country that I think has only recently begun to be fully appreciated for the amount of access it creates for people who have often been considered unserved,” said Missouri Republican Roy Blunt, a Senate co-sponsor.
Minnesota Democrat Amy Klobuchar included an expansion of the program in her broad platform to address mental health and addiction released Friday. The list of co-sponsors in both chambers is bipartisan and in the Senate is split 50/50 between Republicans and Democrats.

‘Keeping people out of jail’
Since the program is only two years old, it’s too early to tell if investments in the new treatment settings lead to savings elsewhere. Yet early evidence from states participating in the pilot program is promising, and the states are eager to continue it.
The three providers Oklahoma certified to receive the enhanced funding have 19 locations serving 17 counties. In the first year of the program, the state estimates that around 23,000 individuals were served, including 11,000 Medicaid beneficiaries.
Oklahoma’s experience seems to be paying off. One of the certified clinics, Grand Lake Mental Health Center, began making investments to expand services in 2015, before the demonstration project. In its seven-county service area, the number of inpatient psychiatric admissions decreased from 1,115 in 2015 to just 15 in 2018, according to Charles Danley, Grand Lake’s chief executive. He attributes the decrease entirely to the CCBHC model, since first responders handling mental health crises previously had nowhere else to go but emergency rooms.
“We were trying to create alternatives to hospitalization. … With the CCBHC, we are able to provide quicker access to services,” he said.
“I can’t fathom it not being continued,” he added.
Oklahoma’s law enforcement officials also seem to appreciate the effort. James Willyard, assistant chief of police in Pryor, said the program has saved his department “thousands of dollars and thousands of man-hours.”
“It’s keeping people out of jail and getting the treatment they need,” he said at the Capitol Hill press conference announcing the bill.
Each state has selected a variety of measures for determining whether the program has been a success, including the number of people served, how long it takes new patients to receive an evaluation, whether emergency and hospital visits have been reduced, how long it takes for the clinic to follow up with a patient after an emergency room visit, and the number who enter and remain in long-term substance use treatment.
But DJ Jaffe, an advocate whose work focuses on those with serious mental illnesses like schizophrenia, questions whether the CCBHC system will be able to help the most difficult cases. He argues that the mental health care system generally focuses on those with easier-to-treat, less expensive conditions. He fears the same could be true with CCBHCs, and while he supports continuing the eight-state program, he cautioned against expanding the program until more evidence is generated.
“Extending them is OK, because there really hasn’t been that much time, they need more time,” he said. “Creating more of them is problematic, though. You don’t want to expand the number of programs until you show the ones that you started work.”
Most of the states contacted weren’t able to provide information about the diagnoses of patients treated by their clinics. But in New York, out of 46,000 individuals treated, 83 percent had a serious mental illness, according to the state’s Office of Mental Health. Compared to previous years, the service areas have seen an 11 percent decrease in emergency room admissions related to behavioral health, and a 26 percent decrease in behavioral health visits requiring an inpatient stay.
Charles Ingoglia, senior vice president at the National Council on Behavioral Health, acknowledged the concern that prospective payment models can encourage providers to skimp on their costliest patients. But in the demonstration states, he said, the fact that inpatient stays appeared to be decreasing in the CCBHC service areas suggested that wasn’t happening.
“The CCBHC has to serve everybody regardless of their ability to pay,” he said. “So it’s not like they could stop seeing that person.”

Keen on expansion
The bill to renew and expand the program was introduced in mid-March. Its sponsors say it’s crucial to give the experiment more time to show its worth.
“We are confident that if we can extend the current eight states for two more years and add additional states, that they will be able to demonstrate to their governors and local communities that this not only works and is right for people but it saves dollars by integrating health care and mental health,” Michigan Democrat Debbie Stabenow, the lead Senate sponsor, said at a March press conference introducing the bill.
The program was originally established as part of a 2014 law mainly meant to delay looming cuts to physician Medicare rates. At the time, the Congressional Budget Office estimated that the first two years of the program would cost around $600 million, and a total of $1.1 billion by 2024. However, paying for the mental health program wasn’t a heavy lift then because the bill contained billions in savings by cutting payments to places like diagnostic labs and hospitals.
John Snook, director of the national nonprofit Treatment Advocacy Center and a supporter of the clinics, described them as “one facility where we do all of the treatment a person needs so I don’t have to send them to one building for one thing and then across town for another.”
He added: “If you were designing a system, this is a common-sense way you would do it. It’s just getting to that point of putting us in a world where we treat mental health like any other illness.”
Supporters of the CCBHC approach say that integrated care results in fewer visits to emergency departments and reduces readmission rates to psychiatric hospitals. People with serious mental illness are also more likely to receive screening or treatments for other conditions, such as blood pressure or diabetes.
The incentive for local governments and mental health practitioners to set up the new facilities came from a rate that is more generous than Medicaid payments, which are typically lower than Medicare or private insurance rates. Medicaid covers more Americans than any other government program and is the single largest payer for mental health care services in the country.
Clinics can get a fixed rate when serving a Medicaid beneficiary, and they are eligible for bonus payments when they meet certain quality care goals, like preventing a follow-up hospitalization, adhering to antipsychotic or depression drugs or engaging in substance abuse treatment. These kinds of “prospective” payments have long been used in Medicare for a variety of services and are meant to encourage providers to focus on quality rather than the quantity of services.
The centers are also able to pay doctors more competitive rates in a field where providers are known to prefer cash to insurance because of the low rates paid by both public and commercial payers. “There’s a shortage of psychiatrists in this country, and if we are not able to offer competitive salaries, we can’t bring them into community behavioral health,” said Heebner, from the Missouri clinic.
In the first few years of the program, HHS provided grants to 24 states to help plan their applications for the full demonstration. The money was spent on developing specific payment models and certifying eligible clinics. Ultimately, 19 states applied, and eight were selected to participate in the two-year Medicaid demonstration. The sponsors of the bill to renew the program suggest the expansion will apply to the 11 states that weren’t selected the first time around.
Backup plans
All eight states are working with the administration on their options to continue the program — even if it means paying for a greater share of it themselves, as some have proposed doing as a contingency if Congress doesn’t act. But for that to happen, the states will need approval from the Centers for Medicare and Medicaid Services.
Walker said Missouri has been working with the Trump administration for more than a year to amend its state Medicaid plan to continue to fund the clinics, with the state picking up the part paid now by the federal government if Congress doesn’t renew the program. The state expects the amendment to be approved before the June deadline so the clinics can continue operating at their current staffing and service levels regardless of whether Congress clears an extension.
The other states participating in the demonstration are also working on amendments or waivers to continue the enhanced payments to the clinics. It’s not clear if or when federal officials would sign off on those.
In Pennsylvania, Maggi Mumma, a spokesperson for the Department of Human Services, said the state “is working with the counties, clinics and behavioral health managed care organizations to develop value-based payment arrangements that could support CCBHC services on an ongoing basis without additional funding from the federal government.”
Oklahoma is also working with CMS on an amendment. The clinics are prepared to go for some time without payment, in hopes they would get retroactive reimbursements under a new law or with approval of a Medicaid amendment, according to an aide to Oklahoma Republican Markwayne Mullin, one of the House bill’s sponsors.





